From: https://www.midwesterndoctor.com/p/how-do-vaccines-cause-autism?utm_source=substack&utm_medium=email
How Do Vaccines Cause Autism?
Past discoveries that can help us understand the current wave of neurological spike protein injuries.
A MIDWESTERN DOCTOR
JUL 21, 2023
One of the most challenging things for me throughout my time in the medical field has been watching children become neurologically damaged by vaccines, and the widespread blindness of the medical profession to this issue. Unfortunately, because so much money has been spent to engineer the societal belief that vaccines do not cause autism, anyone that asserts otherwise is immediately subject to widespread ridicule, to the point it’s mostly a lost cause to convince medical professionals vaccines aren’t always safe. In many cases, the only thing that can open their eyes is their own child being severely injured.
The business of using propaganda (public relations or PR) has gradually evolved into a more and more streamlined formula that reuses the PR techniques found to be the most effective for manipulating the public. Because of this, once the COVID-19 vaccine push started, those who already had firsthand experience with the PR techniques used to prop up the previous vaccinations immediately recognized that something bad was in the works. More importantly, since the exact same vaccine PR scripts were reused to gaslight those with COVID-19 vaccine injuries, it led many to begin questioning the earlier scripts, like those used to debunk any link between vaccines and autism.
The Forgotten Side of Medicine is a reader-supported publication. To receive new posts and support my work, please consider becoming a free or paid subscriber.
Subscribed
Recently
Steve Kirsch started looking at that question, and in an attempt to bring
attention to the issue, raised
three very important points:
1. Contrary to popular belief, there is actually a great deal of compelling
evidence linking vaccines to autism. For example, regressive autism always develops
shortly after vaccination—but never before, something that
cannot happen unless one causes the other. Likewise, there is a significant
amount of evidence correlating vaccine uptake with autism rates.
2. There is presently no accepted explanation for what is causing the explosion of autism we are facing.
3. The explosion of autism is one of the costliest diseases facing our country, so decades of hand waiving that has insisted there’s no scientifically valid explanation for this explosion doesn’t cut it.
You might notice how these three points mirror what we are now seeing with the massive wave of (often unmistakeable) side effects from the COVID-19 vaccines.

Midwestern Doctor @MidwesternDoc
Note: For those interested in learning more about vaccines and autism, I would strongly recommend reading Kirsch’s article. He does a good job of concisely presenting some of the most compelling evidence (e.g., specific cases where vaccination was irrefutably linked to autism and the hundreds of papers on the subject).
One of the major stumbling blocks in proving that vaccines could autism has been to explain their mechanism for doing so. In this article I will start by describing the most commonly cited mechanisms followed by the two‚ I believe play key roles in both vaccines causing autism and the current wave spike protein injuries. Since all of these mechanisms are interrelated, treating one often improves the others.
Vaccine Autism Research
This section was sourced from a compilation of 224 studies that can be viewed here, the book Miller’s Critical Review of Vaccines Studies and Chapter 5 of How To End The Autism Epidemic. Of these, I believe the final book provides the most concise (but detailed)‚ summary of those mechanisms.
Much
of the research on the link between vaccines and autism has focused on the
following areas:
1. Immune activating events being repeatedly correlated with an increased
likelihood of developing neurological developmental disorders like autism.
2.
Increased blood levels of inflammatory cytokines (e.g., “Plasma levels of IL-1β,
IL-6 and IL-8 were increased in children with ASD and correlated with
regressive autism, as well as impaired communication and aberrant behavior”).
Autistic individuals also appear to have a predisposition to developing
inflammatory immune responses.
3. Vaccinations creating inflammation in the brain and inflammation in the
brain being linked to autism. This neurological inflammation is often
chronically active in the brains of autistic individuals and appears to be most
specifically linked to aluminum and the measles virus component of the measles,
mumps and rubella (MMR) vaccine. For example, the vaccine measles virus
was observed to correlate to the production of autoantibodies to brain tissue,
increases levels of measles antibodies were found to
be significantly higher in autistic children (but not antibodies to mumps or
rubella), and live measles viruses were found in
immune cells of autistic children with inflammatory bowel disorders. The
strongest case for the link between the measles vaccine virus and autism came
from the
discovery that vaccines with the measles component have triggered
severe brain injury and death but those with only the mumps or rubella
components have not.
4. Enlarged brains are also often associated with autism (likely due to that inflammation). This swelling may play a key role in the pathology of autism and explain why certain individuals are more susceptible to it.
5. The brain inflammation induced by vaccines occurs at a critical period of brain development.

This argues for providing the vaccines later in a more spaced out fashion; something many have observed dramatically lowers the rate of adverse neurological reactions to vaccines. Unfortunately, safer vaccination practices are never even discussed as doing so would be a tacit admission vaccines are not 100% safe. This is likewise why I believe defenders of the orthodoxy (e.g., Peter Hotez) devote so much energy toward attacking the parents desperately trying to treat vaccine injuries in their autistic children.
6.
Pathologic alterations in the gut microbiome (which increases the likelihood of
autoimmunity), a dysregulated immune response (which includes ones in the
gastrointestinal tract and ones towards a variety of common allergens such as
those within foods), along with a variety of gastrointestinal symptoms being
observed in autistic individuals.
7. The neurotoxicity of mercury, the tendency of autistic individuals to have
elevated mercury exposures, and autistic individuals having difficulty
detoxifying mercury. All of the previous has also be found for lead,
another toxic heavy metal.
8. Aluminum, an inflammatory and neurotoxic vaccine adjuvant, when injected
into mice was found to rapidly
trigger symptoms similar to those observed in neurological developmental
disorders. Aluminum was also
found to trigger a fourfold increase in brain levels of IL-6,
the inflammatory cytokine most closely linked to autism.
9. Aluminum being found in elevated levels in the brains of autistic individuals. For example:
“The aluminium [it is spelled this way in England] content of brain tissue in autism was consistently high. The mean (standard deviation) aluminium content across all 5 individuals for each lobe were 3.82(5.42), 2.30(2.00), 2.79(4.05) and 3.82(5.17) μg/g dry wt. for the occipital, frontal, temporal and parietal lobes respectively. These are some of the highest values for aluminium in human brain tissue yet recorded and one has to question why, for example, the aluminium content of the occipital lobe of a 15 year old boy would be 8.74 (11.59) μg/g dry wt.?”
10. Impairment of the blood-brain barrier being observed in autism (increased permeability of the gut barrier has also been observed).
11. A dose-response relationship existing between specific vaccinations and the likelihood of autism. For example:
The average MMR coverage for the three countries fell below 90% after Dr. Wakefield’s infamous 1998 publication but started to recover slowly after 2001 until reaching over 90% coverage again by 2004. During the same time period, the average autism spectrum disorder prevalence in the United Kingdom, Norway and Sweden dropped substantially after birth year 1998 and gradually increased again after birth year 2000.
12. Likewise, a dose-response relationship exists that has found autism is more likely to occur in premature infants (who effectively receive a higher dose since they are smaller) and those who receive multiple vaccinations simultaneously. For example:
No association was found between preterm birth and NDD [neurological developmental disorders] in the absence of vaccination, but vaccination was significantly associated with NDD in children born at term (OR 2.7, 95% CI: 1.2, 6.0). However, vaccination coupled with preterm birth was associated with increasing odds of NDD, ranging from 5.4 (95% CI: 2.5, 11.9) compared to vaccinated but non-preterm children, to 14.5 (95% CI: 5.4, 38.7) compared to children who were neither preterm nor vaccinated.
Note: This is also the same pattern that has been observed with vaccines causing sudden infant death syndrome (SIDS).
13. A variety of genetic and metabolic abnormalities have been extensively studied in autism. Many of these (e.g., those relating to glutathione) correlate with impaired detoxification and mitochondrial dysfunction, conditions both frequently observed in autistic individuals.
One important thing to understand about these points is the difficulty of identifying a single precise cause autism without a broader picture of what causes it. For example, many were convinced that mercury in vaccines was the primary cause of autism, and there was quite a bit of research that substantiated this link. Yet, despite vaccine mercury being mostly pulled from market, autism has increased rather than decreased since thiomersal (mercury) was pulled.
How Do Vaccines Cause Autism?
In
my eyes, there are three core reasons why vaccines cause autism:
1. They create chronic neurological inflammation.
2. They cause a zeta potential collapse.
3. They create a sustained cell danger response in the body.
Additionally, each of these can cause the other two, making their separation be somewhat arbitrary.
There are a few important correlates of these three processes.
The
first is that things besides vaccines can also trigger each of these occur
(e.g., a congenital rubella infection). The difference with vaccinations
is that they are highly likely to cause each of them and more importantly, are
something (almost) every child is exposed to. As a result, the most
common trigger for autism is vaccination, but other things can also serve as
the trigger for each of these processes. This helps to explain much of
the confusion on exactly what causes autism.
Secondly, these are the same critical processes that underlie many other
diseases such as Alzheimer’s and the myriad of COVID-19 vaccine injuries.
One of the most compelling data points I have come across supporting this
relationship comes from Ed Dowd’s recent discovery of England’s
disability claims data, within which the rate of adult autism
requiring disability support spiked in parallel with the vaccine roll-out:
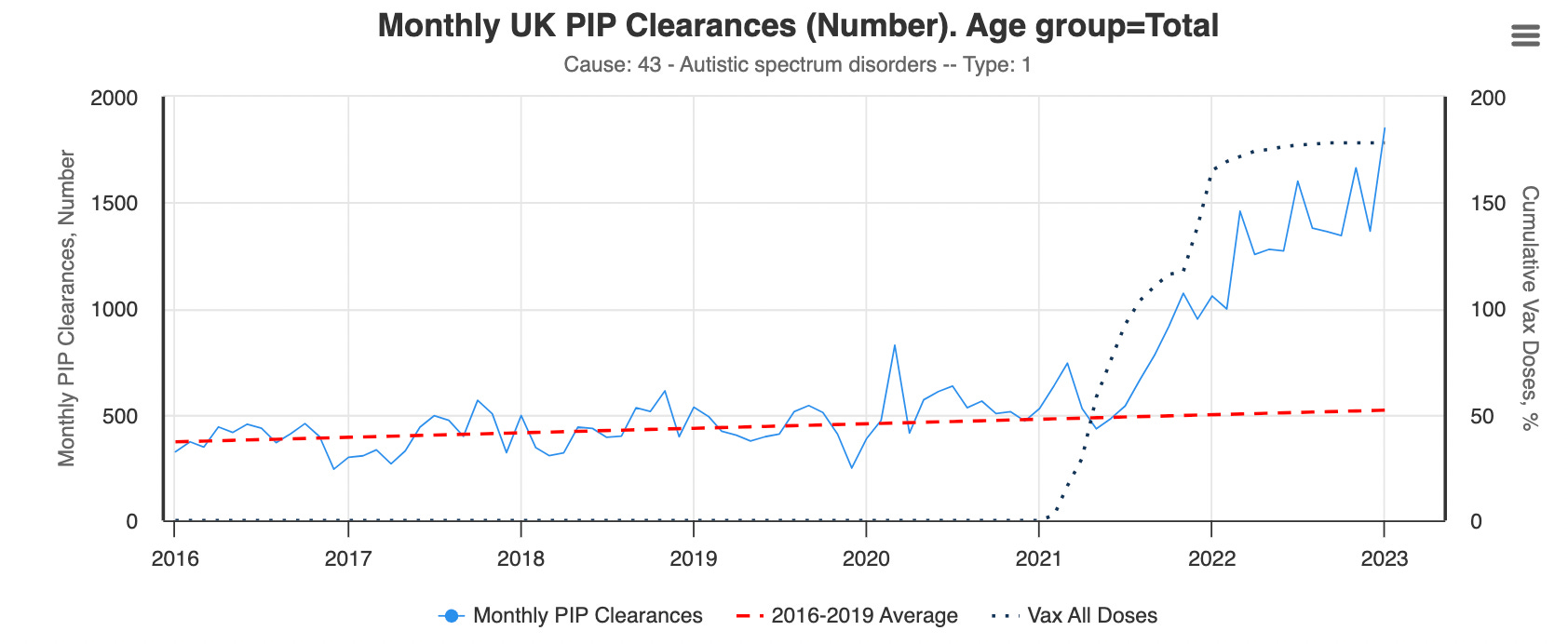
Note: this dataset is for claims in individuals aged 16 and older.
Third, most of the treatments I have seen that effectively treat autism ultimately addressed one or more of these three processes. For example, one large survey of parents with autistic children found virtually all the medications they were prescribed did not help, but four things did:
•Addressing
food allergies (e.g., by removing gluten from the diet).
•Addressing an underlying candida infection.
•Addressing genetically impaired methylation.
•Removing heavy metals from the body.
There are a few other treatments I have also seen significantly improve regressive autism, and I believe each of those treatments likewise improves one of more of the three critical processes. Many of those treatments have also been quite helpful in treating COVID-19 vaccine injuries, so I believe they are even more important to understand now.
Inflammation
The
most common side effect of vaccinations are autoimmune disorders. This makes
sense since vaccines work by stimulating the immune system to respond to
something, and autoimmune disorders result from excessive activation of the
immune system. Although there are many different mechanisms at work here, at
this point, I believe the primary ones are as follows:
1. If the immune system develops an immune response to a target
protein (an antigen) it will often also develop an immune response to other
antigens with similarities to the target antigen, a process known as molecular
mimicry which is well recognized to occur with certain infectious organisms
(e.g., the bacteria which causes rheumatic
fever). Certain vaccine antigens have a higher overlap with human
tissue and hence have a higher rate of autoimmune complications.
Note: one of the major concerns with the COVID-19 vaccines was that its
spike protein antigen had an extremely high degree of overlap with human tissue.
Although this concern was repeatedly raised (e.g., consider this early
2021 paper) it was ignored—much to the detriment of the many COVID-19
vaccine recipients who developed autoimmune complications from the vaccine
(which ranged from 5-25% of recipients depending on the dataset).
2. Vaccines are typically composed of a target antigen under the
theory that exposing the body to the antigen will eventually cause it to
develop an immune response to an infection which also has that antigen.
Antigens tend to be expensive to produce, so it is often not economically
viable to produce enough of the antigen for each vaccine to elicit the needed
antibody response.
There are two common solutions to this approach. The first is to create a
self-replicating antigen (e.g., with an infectious virus that contains the
antigen or an mRNA gene therapy) so enough of the antigen is produced to
solicit an immune response. The second approach is to use an adjuvant—a cheap
compound like aluminum that provoked the immune system to attack anything there
and thereby significantly decreases the amount of antigen needed and thus the
cost of the vaccine.
The
problem with adjuvants is that they will also often provoke the immune system
to develop undesirable responses as well (e.g., allergies
to pollens circulating at the time of vaccination or autoimmunity to
human tissue resembling parts of the vaccine antigen).
3. In medicine, it is often expensive and time consuming to prove a
medication will yield a long term benefit. For this reason “surrogate markers,”
changes which appear quickly and are assumed to correlate
with improved health benefits are evaluated instead. Unfortunately, in many
cases, changes in surrogate markets do not actually correlate with a tangible
benefit.
In
the case of vaccines, the surrogate marker is antibody formation. This creates
a situation where vaccine manufacturers do whatever is needed to create an
antibody response—something which can often be highly problematic. For example,
with the HPV
vaccine, a major design problem was it not eliciting a sufficient
antibody response. This problem was “solved” by using a stronger aluminum
adjuvant, which achieved the desired surrogate marker but also had the side
effect of creating an extremely high rate of autoimmune complications in the
HPV vaccine recipients (making it arguably the most dangerous vaccine on the
market prior to the COVID-19 vaccines).
Note: the best summary of the evidence linked vaccines to autoimmune
disorders can be found within this
textbook on the subject.
Since “inflammation” is a relatively well understood topic, I will focus on the
other two processes for the remainder of this article.
The Cell Danger Response
Recently, I wrote a series that:
•First described the cell danger response (CDR).
•Then
explained the existing approaches for treating a persistent CDR
localized to a specific tissue (something which is often necessary to heal
otherwise chronic injuries).
•Then concluded with methods
for treating a systemic sustained CDR (e.g., spike
protein vaccine injuries).
Since a persistent CDR is often the underlying cause of a variety of chronic
illnesses and functional impairments that significantly affect individual’s
quality of life, the CDR both provides a helpful context to understand why so
many different things can cause the same illness and why the same trigger can
cause so many different illnesses, many of which persist years after the
initial trigger has dissappeared. This section is an abridged summary of
those three articles on the CDR.
When
cells are threatened by something in their environment, they will often switch
to a defensive mode where the cells attempt to protect themselves rather than
performing their normal functions. This process is orchestrated by the
mitochondria, who switch from providing the energy to power the cell into an
inflammatory form that produces the metabolites necessary to defend the cell
from.
When the CDR is triggered, it should go through an inflammatory phase (CDR1),
which is followed by a proliferative and regenerative phase (CDR2), and then an
integrative phase where the cell gradually resumes its normal function (CDR3)
and then exits the CDR. This cycle is essential for the survival of the human
body, and many therapies work by inducing it to repair tissue. However,
in many cases, when the CDR is triggered, instead of it completing, cells get
trapped in either CDR1, CDR2 or CDR3, leading to chronic illnesses
characteristic of the specific frozen and unresolved CDR phase.
The
CDR model is extremely useful in clinical practice for a few reasons:
•First, it helps to explain many of the mysteries in treating complex chronic
illnesses. A classic example would be that integrative physicians
typically assume the mitochondrial dysfunction they see associated with a
chronic illness is the cause of the illness and hence attempt to treat it by
providing mitochondrial supports, an approach which often either does not work
or worsens the patient’s condition.
Note: Each of the common genes known to strongly increase the risk of autism
can be shown to play a role in CDR signaling or maintenance. This helps to explain
why so many different genes have been found to be connected to autism and why
they did not typically cause autism until the trigger of mass vaccination was
also present. Likewise, the wide range of metabolic abnormalities seen in
autism overlap with the metabolic changes created by the CDR.
•Second, a sustained CDR is often the primary cause of autoimmune disorders.
This is an extremely important but relatively unknown fact. Conversely, factors
known to trigger autoimmunity (e.g., an immune stimulating event) often are
also “dangers” to cells that trigger the CDR.
•Third, many degenerative conditions (e.g., Alzheimer’s or a non-healing
tendon) result from cells being trapped in a dormant state where they shut down
and thereby neither heal nor resume their normal function. As a result, regenerative
medicine’s trick for treating many different chronic conditions
characterized by a dramatically reduced functionality of the body is to “wake
cells up out of the CDR.”
•Finally, the CDR helps guide how to treat chronic illnesses and how to
recognize which things are important to address and which should be left alone
because they are simply the result of the body’s compensation to an underlying
issue.
Note: I primarily reference the work of Dr. Robert Naviaux. Others have also researched the process Naviaux termed the CDR and given it different names.
Autism
for instance is characterized by cells trapped in the CDR, and many of the most
successful approaches I’ve seen used for treating autism all treat the CDR.
Naviaux in turn conducted
multiple studies demonstrating that one pharmaceutical drug blocked the
CDR, and when used in autistic animals and then human beings, significantly
improved the condition while the drug remained active—a result that to my
knowledge has never been found in clinical trials of any other therapy for
autism. Sadly, despite years of research on this subject, the drug is
impossible to obtain in America.
Note: excluding Naviaux’s approach, every method I have seen which I believe
effectively improved autism was never feasible to test in a formal clinical
trial.
My renewed interest in the CDR arose after I saw rapid improvements in long
COVID and vaccine injured patients (e.g., someone who had been on oxygen for
months no longer needing oxygen within minutes) from one of the treatments we
previously had had success treating severe COVID-19 cases with. I spent a while
trying to figure out why that improvement could be occurring, and eventually
concluded it had to be because an unresolved CDR was being rapidly resolved.
Since the CDR is known to be triggered by toxic dangers to cells (e.g., the
spike protein), especially after repeated cellular exposures to a danger (e.g.,
from synthetic mRNA that persists in the body and continually produces new
dangerous spike proteins), this seemed plausible. After I contacted a few
leading experts in this area, they all told me their vaccine injured patients
were characterized by a sustained CDR that could not resolve on its own. I then
asked around more and found out that the
same approach we were using to treat the CDR in
spike protein illnesses was also treating a variety of complex (and otherwise
impossible to treat) autoimmune disorders. It also took a bit longer, but I was
eventually able to also find clinicians who were using it to treat autistic
children and each reported remarkable improvements from it (much of which they
had video footage to corroborate).
For all of these reasons, I believe a sustained CDR trigged by the danger vaccines present to the body is a core component of autism (immune activating events trigger the CDR). However, while addressing the CDR can often significantly improve conditions it causes, the benefit is often temporary unless the underlying cause is addressed so the cells no longer have a need to reenter the CDR.
Zeta Potential
Most fluids in nature are colloids (particles suspended in water). With a colloid, two factors are always at play: forces that clump the colloid’s particles together and forces that separate (disperse) them. In most cases, the primary determinant of a colloid’s dispersion—quantified through zeta potential—is if the negative charge surrounding each particle is sufficient to prevent those particles from clumping together.
Since the fluids within the body are colloidal systems, once the zeta potential is no longer sufficient to prevent clumping (agglomeration), the fluids to varying extents solidify and create a variety of problems for the body. This is the easiest to understand with blood, as when the zeta potential declines, blood cells will separate from the plasma, clump together and stop flowing with the circulation.
At this point, I believe the physiologic zeta potential is one of the primary determinants of health. This is because many different diseases (particularly those which cause one to get hospitalized) result from impaired zeta potential, and that many of the consequences of aging come from a gradual impairment of the kidney’s ability to maintain the physiologic zeta potential. In my own practice I’ve found treating zeta potential is often one of the most useful things I can do for patients who show up, so the applications of this concept are very broad.
When I started studying COVID-19, I realized that the disease had all the clinical signs of being extremely disruptive to the physiologic zeta potential of the body (which I believe was why COVID-19 was often so dangerous). After more research, I concluded that this was likely due to there being a strong positive charge on the spike protein, and since then have found papers corroborating this theory and that restoring zeta potential is often critical for treating both COVID and COVID vaccine injuries.
The individual who first linked vaccine injuries to poor zeta potential was Andrew Moulden. Moulden was a Canadian Neurologist (and psychiatrist) who also had an extensive research background (e.g., a Masters and PhD) in the neurocognitive development of children and adolescents, behavioral disorders, neurobehavioral assessment of brain, and detecting acquired brain injuries.
Moulden observed that children who were vaccinated would frequently present with neurological signs of a having had a stroke following vaccination; unfortunately while those signs would often be recognized in adults, they were typically ignored in children. Likewise, I have seen many of the same injuries he described in children (especially abducens nerve palsy’s) develop in friends of mine who received the COVID-19 vaccine.
To try and explain these observations, Moulden drew on decades of previous research into blood clumping and the various diseases it caused (discussed here). He concluded that vaccines diminished the zeta potential of the recipient, causing their blood to clump together and obstruct the circulation of regions of the brain with the weakest blood supplies, thereby triggering microstrokes that were too small to detect with conventional imaging techniques. Additionally, he found evidence suggesting the microstroke issue was worsened by immune activations because white blood cells (which are larger than red blood cells) would migrate into the small blood vessels and obstruct their flow, something he termed MASS.
Moulden then mapped out the most common micostrokes that would occur (due to the nature of their blood supply). In this, noticed that many children who developed severe neurological disorders like autism simultaneously showed clinical signs of having had microstrokes, leading him to conclude those microstrokes were causing a variety of brain injuries, including autism and SIDS.
One
of the most important things about Moulden’s model was that like the CDR, it
was a universal mechanism of harm and things besides vaccines (e.g., a
congenital rubella infection) could also cause those dangerous microstrokes to
happen. Additionally, certain vaccines (Gardasil, Anthrax and
I would argue the
original Smallpox vaccine) had a much greater
propensity to cause the same microstrokes that the COVID-19 vaccines have now
made us all aware of.
Conversely, those who already had an impaired zeta potential were the ones most
likely to have severe reactions to vaccines because they could not tolerate
additional impairment of their physiologic zeta potential. This for example
characterized the patients I have seen who were admitted to the hospital for a
complication caused by a traditional vaccine and why the elderly (who have a
baseline impairment of their zeta potential) are so much more vulnerable to
conditions like the flu which consistently worsen the physiologic zeta
potential, hence bringing vulnerable individuals past the agglomeration
threshold that they can tolerate.
Note: After discovering this mechanism of injury, Moulden switched his focus to trying to treat it, but shortly before he had planned to release his treatment died unexpectedly and many have since tried to figure out what he had discovered. Based on studying his work and talking to friends who knew him shortly before his death, I believe Moulden’s approach was based around restoring the zeta potential of vaccine injured children, something which is much easier to do with the tools available now than those that were known when Moulden was still alive.
My colleagues who actively work with the CDR in practice believes it goes hand in hand with zeta potential and that the CDR often cannot be treated unless the fluid stagnation inside a patient is addressed (e.g., Lyme and mycotoxins both frequently cause stagnation because their positive charges impair zeta potential). Furthermore, in many cases, the loss of blood flow to, or drainage from tissue can be sufficient to trigger the CDR. In general, my colleagues believe one of the biggest treatment oversights made by integrative doctors who work with complex illnesses is the doctor’s failure to address the lymphatic stagnation that results from a zeta potential collapse in their patients.
Note: While treating the CDR will improve many symptoms of a disease, especially if the trigger of the CDR (e.g., a chronic infection) is still present and treated as well, treating it will not address existing damage, such as that previously caused by microstrokes. This is why the animal studies Naviaux conducted found his drug improved many symptoms of autism but did not improve those resulting from damaged and lost brain tissue. Likewise, my colleagues have found many of the core symptoms of autism can be improved with approaches directed at the CDR or Zeta Potential which reactive dormant brain cells, but it is much more challenging to treat specific neurological deficits resulting from previous microstrokes.
I
also believe impaired zeta potential goes hand in hand with autoimmunity. This
is because:
•The existing diagnostic system that best encapsulates impaired zeta potential
is “blood stasis” from Traditional Chinese Medicine. TCM links blood stasis to
a variety of autoimmune conditions.
•Lymphatic stagnation will cause autoimmunity. I believe a key reason why blood
stasis is linked to autoimmunity is because lymphatic stasis will exist in
parallel to blood stasis as both result from the same impaired physiologic zeta
potential.
•Inflammatory states (as shown by the ESR test) reduce the zeta potential of
the blood.
•Inflammatory activation triggers MASS which creates microstrokes, especially
in the setting of poor zeta potential.
•Aluminum, the most commonly used vaccine adjuvant, is also the element with
the greatest adverse effect on zeta potential (aluminum’s coagulating ability
is orders of magnitude greater than any other element).
•I suspect aluminum’s ability to disrupt zeta potential is why it functions as
such an effective adjuvant. This is because many infectious organisms also
create a localized disruption of zeta potential and hence any disruption of
zeta potential serves as a universal signal to activate the immune system.
Note: one of the reasons why aluminum is so problematic is because
macrophages will treat it as an invading microbe and eat it. However, since
they cannot digest it, the macrophages will keep the aluminum inside them and
eventually deposit it in specific parts of the body (e.g., where the macrophage
eventually dies).
For reasons that are not fully understood, the macrophages predominantly concentrate aluminum in critical tissues in the body (e.g., the brain and spleen) and are more likely to do this when smaller doses of aluminum are used, thereby allowing a small dose of aluminum to become a toxic dose. A major problem with both aluminum and the mRNA gene therapies is that they don’t obey the classic assumptions in toxicology (e.g., that toxicity increases directly in proportion to the initial dose).
Presently,
I believe the reason why both zeta potential and the CDR are such frequent
causes of chronic illness is because each evolved in an era when we had far
less stressors on our system. In the case of the CDR, while protective, if it
is repeatedly triggered, it becomes more likely for cells to become stuck in
the CDR. While an increasing sensitivity to environmental dangers was helpful
in the past, since we are now exposed to too many triggers for the CDR, many
are now to varying degrees trapped in the CDR.
In the case of zeta potential, the body ideally wants to have a zeta potential
slightly above the threshold that will cause blood clumping and then clotting
to occur, as this saves you from otherwise fatal bleeds. However because we are
exposed to so many zeta potential disrupting toxins (e.g., the aluminum throughout
our environment), the negative charge our bodies evolved to contain is often no
longer are sufficient to keep us above the critical agglomeration threshold.
Furthermore, I believe the three mechanisms outlined here, inflammation, an unresolved CDR, and impaired zeta potential are also the primary causes of aging. To this point, one of the most common side effects of a COVID-19 vaccine injury are those individuals reporting that it seemed as though their bodies had aged significantly, something also observed by pathologists who had performed autopsies on individuals killed by the COVID-19 vaccines.
Conclusion
Many have argued an epidemic of neurological and autoimmune disorders characterize the modern age. For example:
Under Dr. Fauci’s leadership, the allergic, autoimmune, and chronic illnesses which Congress specifically charged NIAID to investigate and prevent, have mushroomed to afflict 54 percent of children, up from 12.8 percent when he took over NIAID in 1984.
One of the primary culprits for this change was Fauci brokering a 1986 deal that incentivizing a flood of unsafe childhood vaccines to enter the market:
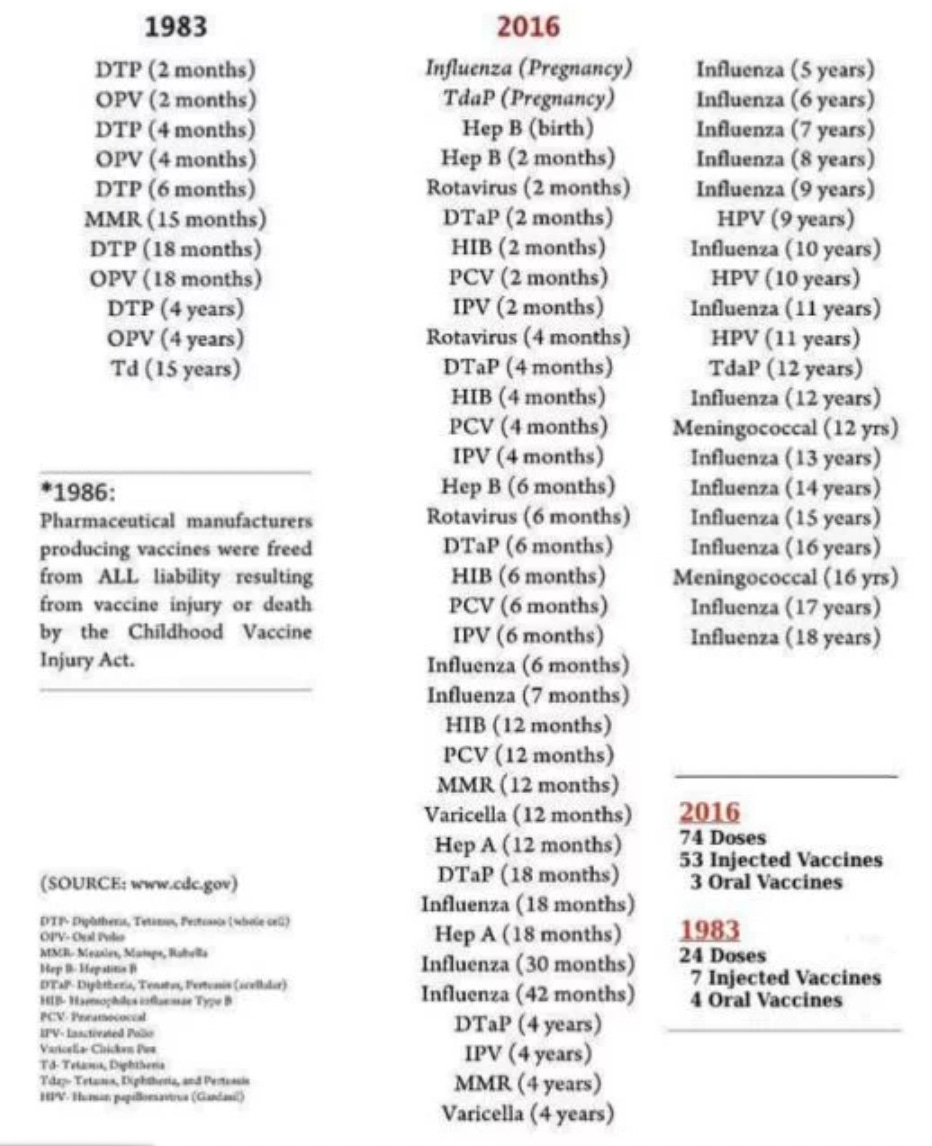
Note: the vaccine schedule has since been updated to include unjustifiable childhood COVID-19 vaccinations. It is not yet clear how many doses of those will be required (presently its 2-3 but COVID-19 could easily become another annual vaccination).
Typically when a pharmaceutical harms someone, it is relatively subtle and hence hard to recognize. The best way I can think to describe the process is with this graph:

Normally, we would depend on large research studies to
determine if a pharmaceutical was in fact causing “moderate reactions.” Unfortunately,
because of the systemic corruption in medical science, data showing a lucrative
pharmaceutical is harming large numbers of people almost never gets published.
Instead, we often can only recognize the
presence of severe and unmistakable reactions (such as the epidemic of
sudden deaths in healthy athletes) to clue us into the harm of a
pharmaceutical. Those severe reactions are critically important to recognize
because as the above curve shows, they are the tip of the iceberg and indicate
a much larger number of less severe reactions are also occurring.
For
example, while the COVID-19 vaccines are well known for causing fatal blood
clots in the brain, what is less appreciated is the widespread effects they
have had on general cognitive function (something generally recognized to
decline with age as a result of poor blood flow to the brain). Many people
(including numerous physician colleagues) I know have reported cognitive
impairment following COVID vaccination and I have likewise observed this in
many colleagues who still support the vaccine. Likewise, now and then I hear of
significant cognitive decline in an elderly individual after they received a
traditional vaccination.
Recently, I learned that the Netherland’s healthcare system had discovered that
since the COVID vaccines rolled out, there
was a 24% increase in doctor visits for memory and
concentration problems in adults (the increase varied from 18%-40% depending on
age). This is an absolutely massive increase (discussed further here), and helps to illustrate a real life example of the pharmaceutical injury
bell curve.
The individuals who are more sensitive to toxins (and likely to have a severe reaction) are often referred to as “canaries in the coal mines.” It is my belief that if as a society we considered the severe reactions those canaries had experienced from pharmaceuticals rather than ignoring or gaslighting them, the health of the nation would be dramatically improved since we would not have to deal with the much larger number of moderate injuries hidden within the bell curve.
Autism is one critical example, as the severe regressive cases caused by vaccination represent the visible extremes of the injury while far more moderate neurological injuries from vaccines also occur throughout the population (including less severe forms of autism—hence why it now is termed “autism spectrum disorder”). For example, many of the same mechanisms that cause autism, when instead allowed to work over a slower period are the most likely causes of Alzheimer’s disease (e.g., elevated aluminum concentrations are also found in those brains). Likewise, one of the common tragic COVID-19 vaccine injuries is rapid cognitive decline in elderly individuals following their vaccination, which is then typically written off as Alzheimer’s and never further investigated.
Like autism, many effective treatments exist for Alzheimer’s disease (e.g., treating the CDR or restoring fluid circulation to the brain), but since none of them revolve around utilizing lucrative drugs, they have all been swept under the rug. It is my sincere hope that the need to address the severe consequences of the COVID-19 vaccines throughout the population will make the world be open to looking at the much broader consequences of the vaccination program and what can be done to heal the ever-increasing damage it has inflicted upon society.
Lastly,
something recently changed in Substack and I’ve begun receiving individual
messages from subscribers each time they signs up to financially support this
publication—to each of you, I’ve taken your kind words to heart and they’ve
given me a lot of thoughts on how I can best structure this newsletter for
everyone.
I sincerely thank each of you for your support, the time you’ve taken to make
sense of these concepts laid out in this article, and your help in to getting
the information to those who can most benefit from it.
The Forgotten Side of Medicine is a reader-supported publication. To receive new posts and support my work, please consider becoming a free or paid subscriber.
Subscribed
This post is public so feel free to share it (e.g., on Twitter)